




Eugenia Victoria Ellis, PhD, Elizabeth W. Gonzalez, PhD, APRN-BC, and Donald L. McEachron, PhD
Abstract
Evolutionary processes generate a variety of paradoxes which must faced in order to design the most effective structures to fulfill various human requirements and preferences. One of these paradoxes comes from the evolution of circadian rhythm systems, which are normally synchronized to the geophysical cycle of night and day and coordinate internal temporal order, now in conflict with modern technology and the 24/7 paradigm for urban living. Modern lighting systems have traditionally focused on providing sufficient illumination for people to navigate and manipulate their environments without regard to the side effects that lighting might have on temporal aspects of behavior and physiology. However, studies involving shift work and other applications of artificial lighting have indicated that these side effects can be quite significant. Further, when an aging circadian system is coupled with a deteriorating physiology the side effects of a 24/7 artificially-illuminated indoor environment can be especially debilitating, especially for older adults with dementia. Chronobiology is the field of biology that examines periodic (cyclic) phenomena in living organisms whereas photobiology is the scientific study of the interactions of light on living organisms. Chronobioengineering (McEachron, 2012; Halberg, 1997) is an emerging field of scientific study that translates research results and concepts from these fields into practical applications.
The following discussion focuses on the use of light cycles to synchronize circadian rhythms and ways human health and well-being can be enhanced through LED lighting in the aging population, specifically those with dementia of Alzheimer's type. The hypothesis is that the implementation of a lighting system specifically designed to synchronize circadian rhythms in this population will alleviate symptoms of dementia and thus enhance the quality of life for both residents and care-givers. The research team is working with a lighting industry partner to manufacture a 2'x2' retrofit LED luminaire for installation at St. Francis Country House, a skilled nursing facility near Philadelphia. Research includes working with the nursing home caregivers and administrators to establish criteria and protocols for the Evidence-Based Design research that will evaluate the efficacy of the daylight-matching luminaire.
The Evolutionary Paradox – Implications For Architectural Design
The process of biological evolution is primarily dependent on the twin mechanisms of random mutation and natural selection. Evolution proceeds by way of increasing and decreasing gene frequencies over generations, irrespective of how these changes are produced. Thus, it is possible - and often observed - that the wellbeing of individual organisms is sacrificed in order to promote gene transmission. As a consequence, evolutionarily determined physiology and behavior may or may not promote the welfare of the individual processing those traits. Second, random mutation does not necessarily create the best adaptations even when those adaptations would benefit gene propagation. The process of creating new mutations is random relative to the requirements of gene proliferation and thus quite sensible adaptations may never evolve. Third, organisms are always best adapted to their ancestors' environment. It is the ancestors who succeeded in propagating their genes over time and not the current representatives. Although rapid evolution is possible, significant change is dependent upon generation time and organisms with relatively long generation times – such as humans - take longer to adapt to new conditions, at least biologically. Fourth, emotions are part of evolution and thus likely to be one method by which genes promote behaviors that result in their own dissemination. These observations and arguments lead inevitably to the conclusion that human beings retain an evolutionarily determined mixture of biologically maladapted traits and behaviors ill-suited to the current urban environment. Understanding these biological limitations is one key to creating the best internal ecosystems, for both individual building occupants and for the larger community.
Current structures are also cultural artifacts, dependent on a number of complex social and economic systems that have grown up historically in relation to the ways that humans use resources - water, building materials, various technologies (ex. electricity), and rules (building codes, zoning laws, etc.). Such factors can result in unintended, and often overlooked, negative consequences for building occupants.
These observations have not gone unnoticed by architects, engineers and researchers. In 1992, Chevan suggested that both productivity and health could be linked to design features, while Kilbert and colleagues (2000) argued for an ecological approach to building construction and design, a call echoed by Berry and coworkers (2004). Samet and Spengler (2003) stated that a "more comprehensive rethinking is needed on the physiological, sociological, ergonomic, and psychological characteristics of the built environment that affect health and well-being." Mitchell and coworkers (2007) called for more research on the effects of building design on human health while Khalid (2006) claimed that knowledge of the interaction between design and affect (emotion/mood) would be required to accommodate a diversity of occupants. In arguing for neuroscience research to be used to inform building design, Edelstein (2008a) also touched on the theme of diversity. She suggested the creation of 'environmental zones' to accommodate the changing needs of various users across time, space and according to task. Wang (2009) provided data in support of variable environmental requirements by demonstrating that maximum productivity and most preferred environmental conditions did not always match in his subjects. Calls for the application of new evidence-based, human-oriented designs have been made for offices (Chevan, 1992; Ford, 1973), medical facilities (Edelstein, 2008b; Berry, 2004) and schools (Rydeen, 2008). In all these situations, there is a need for an adaptable and evolving internal ecosystem capable of adjusting for different occupants, variations within occupants and for differing tasks. In the case of aging populations, especially those with dementia, these issues can become critical. This paper investigates an emerging field – chronobioengineering – that seeks to create environments which promote temporal health. Improvements in temporal health, in turn, may help to alleviate symptoms of dementia in older adults living in a long-term care facility.
The Time Machines – Rhythms And Oscillations In Biological Systems
Temporal health is a matter of temporal order – the right events occurring in the right order at the right time. All biological organisms depend on rhythms and oscillations to time critical activities. When timing is disrupted, systems begin to fail. One example of this is the phenomenon of jet lag, a temporary reduction in the efficiency of physiological and behavioral processes after travel across several time zones. More severe consequences are associated with shift work, where there are longer and more significant insults to the biological timing system. The majority of studies investigating the effects of shift work report a variety of behavioral and physiological issues associated with this form of temporal disruption. Physiological issues include sleep disruption, reproductive problems, gastrointestinal complaints, metabolic abnormalities, enhanced danger of cardiovascular problems and an increased risk for certain types of cancers. Behavioral issues include decrements in cognitive performance, depressed mood, psychiatric complaints and increased reports of neuropsychological problems (McEachron, 2012; Davis and Mircik, 2006; Haus and Smolensky, 2006; Davis, 2001; Costa, 1996; Harrington, 1994)
So, temporal health clearly matters to human health and well-being. However, how do these data apply to the situation at hand – the residents of a long-term care facility? Why should architects be concerned with jet lag and shift work in the design of what appears to be a fairly stable environment? To understand this requires a bit more information on how the human biological timing system actually works.
A major factor controlling human biological timing is the circadian rhythm. Circadian rhythms are endogenous (self-generated) biological rhythms produced by specialized cells or structures which impose a near 24 hour period on the physiology and behavior of individual organisms. The adaptive function of such rhythms is to position the organism's behavior and physiology within the geophysical cycle of day and night. To accomplish this task, circadian rhythms cascade throughout the entire physiology and biochemistry of the body to coordinate a vast array of other activities and biological oscillations of varying frequencies and functions. For example, there are circadian rhythms in heart rate which reduce the frequency of beats during sleep. When this rhythm does not occur or is faulty is some way, there is an increased risk of cardiovascular damage and heart attack (de la Sierra, 2010). Thus, in order to be effective, the circadian rhythm system must maintain an internal temporal order that coordinates an organism's activities at every level.
In constant conditions without an external light/dark cycle or other environmental indicators of time, circadian rhythms express their inherent, internal frequencies that typically vary slightly from 24 hours. These so-called free-running rhythms are usually only seen under laboratory conditions but can be observed in some blind individuals unable to process lighting information. Virtually all aspects of an organism's behavior and physiology are linked to the circadian system and will free-run under constant environmental conditions.
Normally, organisms are not exposed to constant environmental conditions but rather time-varying levels and wavelengths of light as well as other environmental variables linked to the Earth's daily rotation. It is clear from innumerable observations under both laboratory and field conditions that light/dark cycles are capable of synchronizing circadian rhythms. In other words, when an organism with a free-running circadian rhythm different from 24 hours is exposed to a light/dark (LD) cycle of 24 hours, the circadian rhythm changes its period to match that of the LD cycle, i.e., displays a period of 24 hours.
The Circadian System in Humans
As mammals, the main pacemaker controlling circadian rhythms in humans is located in the suprachiasmatic nuclei (SCN) in a brain region known as the hypothalamus. The SCN are circadian clocks that provide circadian information to all cells in the body to adjust their physiology according to the time of the day (Pittendrigh, 1993). The SCN maintains and regulates the 24-hour rhythms of physiological and behavioral systems, by either directly driving those rhythms or indirectly through synchronizing secondary oscillations that are then responsible for the biological cycles (Vujovic, 2008; Hastings, 2003). The existence of this internal entrainment network means that any disruption of the signals coming from the SCN can release control over multiple secondary oscillators, leading to numerous independent rhythms and a loss of internal temporal order. Such a disruption can either be brought about externally, from inappropriate lighting information or other conflicting environmental signals, or internally, from a loss of SCN function or other neurological issues.
Lighting information sent to the SCN which measures lighting time and intensity comes from a unique sensory apparatus in the retina, separate from the organization of rods and cones associated with standard vision – object recognition, color vision, motion detection, etc. This alternative system is based in the intrinsically photosensitive retinal ganglion cells (ipRGC) – the neural processing units of the retina – and the pigment associated with light absorption displays a slightly different absorption spectrum from that typically of the rods and cones (Berson, 2002; See Figure1). Practically speaking, this means that while photopic light supporting vision and light informing the circadian system overlap, it is possible to differentiate these effects on the basis of wavelength and design lighting systems that provide visual support while minimizing inappropriate timing input to the circadian system.
In a natural environment, light reaching the retina is processed by these ipRGC and the information is transmitted to the SCN where the information changes the state of the SCN neurons. This change involves a phase shift of the ongoing oscillations. When light is provided as a sinusoidal wave with gradual onset and offset and sufficient amplitude, the effect of the lighting cycle is to synchronize or entrain the oscillations of the SCN. The SCN, in turn, through various mechanisms entrains the rest of the many oscillators distributed throughout the body. Thus, the optimum condition is a sinusoidal light cycle of 24 hours entraining the SCN and the SCN then imposing temporal order on the remaining physiological and cognitive processes.
What constitutes a natural environment? Light can be expected to display a gradual increase in lighting (sunrise) and powerful, sustained lighting (daylight) and a gradual decrease in lighting (sunset) followed by a profound darkness (night). These effects involve both intensity and wavelength variations in perceived lighting. Focusing on illuminance alone, a moonless overcast night may provide only about 10-4 lux, while full daylight provides 10,000-25,000 lux and direct sunlight 32,000–130,000 lux (http://stjarnhimlen.se/comp/radfaq.html - 10). The actual levels depend on both latitudinal location on the Earth and weather conditions, but clearly the circadian system evolved to expect a dynamic range of lighting over some 6-9 orders of magnitude.
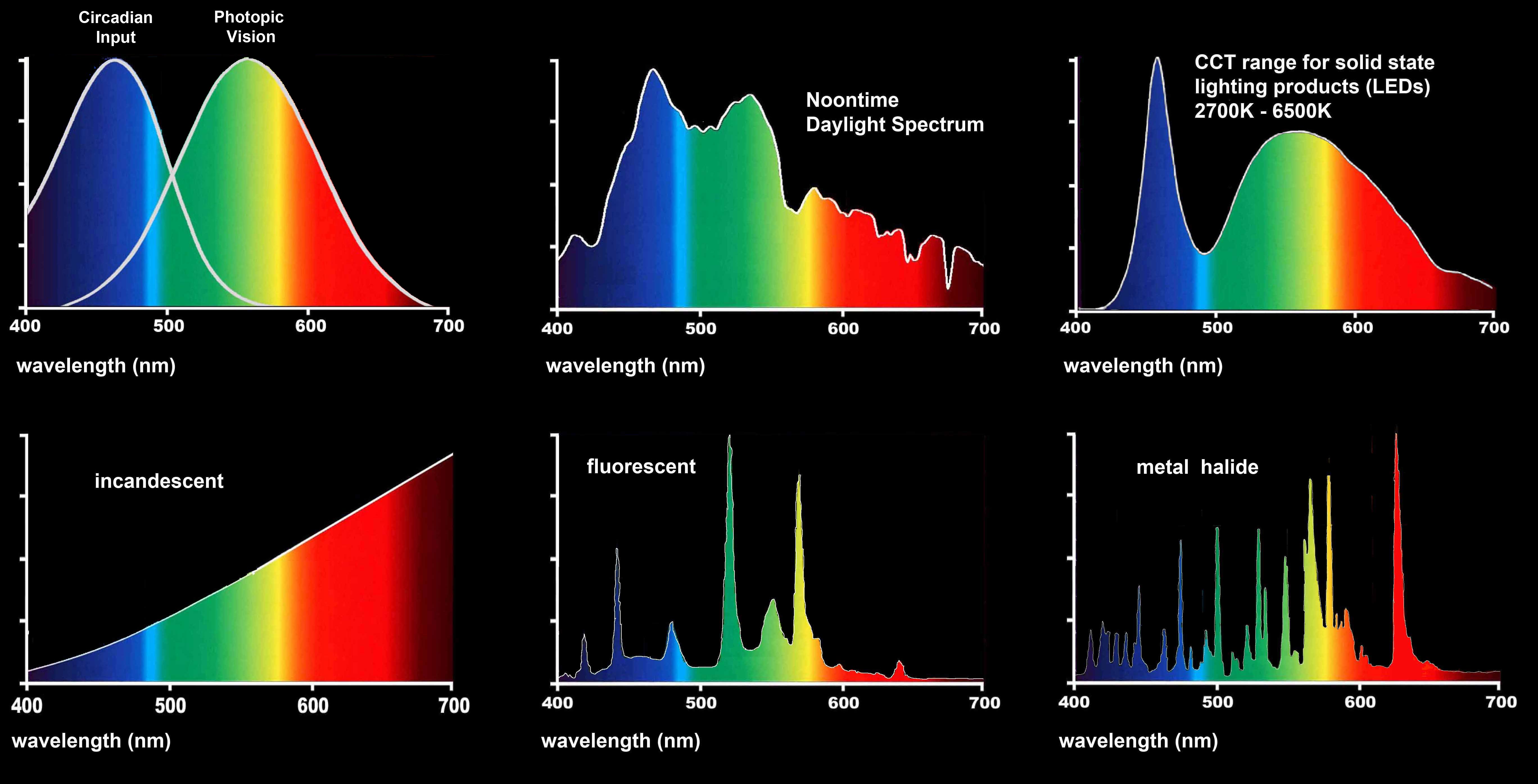
Figure 1. Light Spectrums Associated with Vision and Circadian Timekeeping (adapted from Brainard, G.C. (2009) Presentation to American Society for Photobiology). What is perceived as "white light" from the sun is actually comprised of the full spectrum of colors. Circadian reception occurs primarily in the blue-green range (446-477 nm, Brainard, 2001). LED sources of mixed RGB (red, green, blue) and white LEDs allow for dynamic control of color (DOE, 2013). Compared with either electric filament (incandescent) or gas lamps (fluorescent, metal halide), LEDs have the potential to most closely match the full spectrum of daylight because they are infinitely controllable.
In review, the human circadian organization is based upon a pacemaker located in the SCN and linked to lighting through a specific blue-green sensitive receptor system in the retina. The SCN is entrained to the environmental cycle of day and night through phasic effects and a PRC. Gradual, high amplitude sinusoidal variations of light and dark are more effective at promoting synchronization to the environment compared with abrupt lighting changes which may generate external rhythmic disruption. Such external disruption generates internal rhythmic disruption and a loss in internal temporal order. A loss of internal temporal order is damaging to physiological and behavioral functions. The system is also sensitive to light intensity and photoperiod length effects, all of which must fit together appropriately to generate rhythmic coherence. Such coherence is vital to promote health, wellbeing and productivity.
Light And Perception – The Special Case Of The Elderly
Chronobioengineering is an emerging field of scientific study that translates research results and concepts from photobiology (Roberts, 2001) and chronobiology (Brock, 1991) into practical application. Considering the photobiological effects of light on the body and its circadian significance, the reception of light, especially natural daylight, is of major significance to architects when designing buildings (Ellis, 2011). Further is the design of electric lighting systems for interior spaces that are inaccessible to natural daylight during the day and for facilities that are illuminated 24-hours per day, such as hospitals. The negative effects of nighttime lighting on endogenous circadian rhythms has become such a concern that the American Medical Association has declared it a public health issue (AMA, 2012).
The effect of light on the health of the elderly is a special case because the circadian clock begins to weaken as people age (Sinoo, 2011; Turner, 2008; ANSI/IESNA, 2007; Samis, 1968). As a result, it is critical to maintain an environment sufficient to reinforce 24-hour rhythmicity in building interiors where elderly individuals reside. Unfortunately, the opposite is usually the case. Often, older adults live at home under low-lighting conditions with the shades drawn, while institutional lighting levels are also much too low during the daytime, do not provide residents with the full spectrum of changing lighting levels throughout the day, and do not provide total darkness at night (Burns, 2009; van Hoof, 2008; Aarts, 2005; Schochat, 2000) – conditions that could be changed to help synchronize circadian rhythms to maintain internal temporal order. Creating appropriate conditions in nursing home facilities is difficult to do, especially total nighttime darkness, since caregivers need to work throughout the night monitoring patient health and safety, as well as fulfilling their administrative tasks. Because humans evolved in an environment with a changing spectrum of light throughout the day (including darkness at night) circadian reinforcement becomes increasingly critical as people age and their internal clocks become less reliable. Chronobiologically appropriate lighting may prove to be a significant factor in ameliorating symptoms of dementia, mood and sleep disturbances (Sinoo, 2011; Burns, 2009; van Hoof, 2009; Riemersma-van der Lek, 2008; Sloan, 2007).
How bad is the situation in resident nursing facilities? Remember that the circadian clock evolved to expect a sinusoidal variation in intensity of 6-9 orders of magnitude with a trough near 10-4 lux and a peak between 20,000 – 100,000 lux combined with wavelength changes. One study reported that daily exposure to light of over 1000 lux occurred for nursing home residents for only 9 minutes per day (Ancoli-Israel, 1997). A Canadian report that individuals without sleep problems developed them after being admitted to residential facilities (Clapin-French, 1986) and sleep fragmentation is a major issue among nursing home residents (Regestein and Morris, 1987). Another study found that the amount of light in eight nursing homes was not sufficient to meet the visual needs of elderly residents putting residents at risk for falls (De Lepeleiri, Bouwen, De Coninck, & Buntinx, 2007). Clearly, current lighting environments are not providing adequate chronobiologically appropriate lighting to promote temporal health.
Caring for residents in dementia units of skilled nursing facilities requires additional attention beyond the provision of assistance in activities of daily living (ADL) to elderly residents. The design of the built environment needs to consider various physical and psychological difficulties of individuals with dementia. Residents with dementia can experience the "sundowner's" effect – restlessness, agitated behavior and confusion toward the end of the day – and often have difficulty sleeping at night (Wu and Swabb, 2005). Additionally, such residents often exhibit a need for mobility and a tendency to engage in wandering behavior (Doliansky, 2006). These symptoms reduce the quality of life of individuals with dementia, and their families. Many of these symptoms have been linked to insufficient exposure to light leading to disruption of biological rhythms (Wu, 2007).
While skilled nursing facilities are often designed with specific "sunrooms" for their residents, it is not always possible to bring daylight to building interiors in general. Studies have shown that dementia residents require a minimum of 1000-2500 lux "in the gaze direction," or vertical illuminances, for a significant portion of the day in order to generate a positive effect on rhythms (DOE, 2010; Van Someren, 1997). Standard fluorescent lighting delivers less than half that amount and does not have photonic light levels comparable to the action spectra of natural daylight required for melatonin suppression to maintain circadian rhythmicity. Neither do the other electric filament or gas lamp alternatives (Figure 1). Thus, the characteristic lighting environment of nursing facilities in the day rarely has the intensity of light required by elderly adults. This situation is exacerbated by the operational need to keep lights on at night. As a result lighting is too dim in the daytime and too bright at night to generate an effective timing signal for human biological rhythms, which rely on the amplitude of the day/night differences in lighting to convey time-of-day information to the brain. This lack of an effective environmental timing signal – combined with age-related fragility in the circadian organization of elderly adults (Brock, 1991; Van Gool, 1986; Miles, 1980; Ehert, 1978; Samis, 1978) – unfortunately generates an even more extreme situation for disrupted circadian rhythmicity (Noell-Waggoner, 2006). Designing an indoor lighting environment for older adults to meet this need can be difficult to achieve since engineers characteristically design lighting levels based on horizontal illuminances, or lighting levels at a certain height from the floor such as a table top. Also, illuminances at the eye where the light is actually received by the body are affected by the reflectivity of the surrounding surfaces (walls, floors, ceilings, table tops, etc.) and contingent upon where the building occupant is actually looking (Van Hoof, 2012).
Humans use the entire body as a medium of experience to apprehend the world around themselves (Ellis, 2000). Perception of that world is an active interrogation of the environment through the senses that creates a feedback loop between the body and world (Gibson, 1966). Visual perception especially is dependent upon the experience of the relationships between objects in space based upon the body's relative position in space, which is a haptic and tactile perception (Ellis, 1999). Due to changes in vision, that feedback loop can be interrupted and cause a misstep by the perceiver. This is likely to be more pronounced in the elderly due to changes in vision and the visual system of the aging eye (Torrington, 2007; Noell-Waggoner, 2006) and a major cause of the high incidence of falls among older adults (ANSI/IESNA, 2007).
To be effective, light must be perceived. Unfortunately, the amount of light reaching the retina of the elderly, even those with intact vision (pupils open and reactive), is significantly reduced compared with young adults. By the age of 65, only one-third of that light reaches the retina, by the age of 85, only one-fifth (ANSI/IESNA, 2007; Noell-Waggoner, 2004). Practically speaking, as the need for a high amplitude light/dark cycle increases, the ability to perceive light is being reduced. Other age-related visual changes include: 1) increased sensitivity to glare, 2) longer adaptation time required for changes in brightness, 3) loss of contrast sensitivity, 4) distortion of colors due to the yellowing of the lens or cornea, and 5) loss of accommodation. For adults with cataracts, macular degeneration or blindness, the situation is exacerbated. While a loss of accommodation may be remediated through corrective lenses or glasses, the other five changes in vision must be addressed through the design and lighting of the interior environment (Noell-Waggoner, 2006). As an additional issue, the yellowing of the aging eye scatters out the blue light wavelengths needed to inform and reinforce the circadian system (Turner and Mainster, 2008), requiring higher than normal illumination levels to achieve optimal effect.
Auto-Tuning Daylight With LED Lighting
By replacing traditional artificial lighting with LED luminaires that mimic the full spectrum of natural daylighting, including darkness at night, the hypothesis is that sleep patterns and global functioning of building occupants will improve. To accomplish this, a fully programmed, integrated LED luminaire is being developed to "auto-tune" the color and intensity of natural daylight throughout the day. This would then provide quality illumination for visual tasks and help synchronize biological rhythms for better health, cognitive ability and performance.
While the literature demonstrates that natural daylight has a significant impact on human health and performance (Joseph, 2006), there is no commercially-available luminaire or lighting system designed specifically to improve health outcomes. There are a number of products on the market that claim to supply "full spectrum" lighting (according to Full Spectrum Solutions, "Full Spectrum Lighting is considered to be any lamp with a color temperature between 5000K and 6000K with a CRI of 90+") in the form of compact fluorescent and induction lamp (BlueMax™ HD induction lamp, Lawrence Livermore Laboratories, Berkeley, CA, U.S. Patent #6,318,880) luminaires, as well as a number of "dawn simulators," which are light boxes one can sit facing, but are not indoor environmental lighting systems. These "full spectrum" lighting products can provide consistent lighting levels using the full spectrum of noontime sunlight. Some of these fixtures can be dimmable, but none of these products are capable of actually mimicking the full spectrum of natural daylight in both color temperature and light intensity: the amber of the rising sun, the intensity of the noontime sun with the cast of a blue sky, and the dim amber to red of the setting sun. Neither compact fluorescent nor induction lamp light sources have the ability to change color throughout the day. Incandescent light is closer in color temperature to late afternoon light when blue light is preferentially scattered out of (removed from) incoming sunlight and daylight turns to orange light. While other light sources can be turned off at night, no other light source is programmed to illuminate the indoors throughout the night without disrupting the circadian rhythms of building occupants. Figure 1 shows the light spectrum required to stimulate the circadian system and the noontime daylight spectrum in comparison with various electric light sources.
Through a combination of white and RGB (red, green, blue) LEDs in one integrated luminaire, it is possible to auto-tune lighting to change color throughout the day to mimic the full spectrum of natural daylight from dawn to dusk, changing the color throughout the day from the rising sun to the setting sun and illuminating building interiors with a low-intensity red light throughout the nighttime hours. Further, LED light level conditions can be programmed to accommodate the eye gradually shifting from daytime photopic (cone) vision to nighttime scotopic (rod) vision—a process that takes significantly more time for the elderly. Similar to photosensitive paper, which is not affected by red light in the photographer's darkroom, the body's circadian system is minimally affected by red light in the environment because the intrinsically photosensitive retinal ganglion cells (ipRGC) in the retina are not receptive to red light (AMA, 2012; Brainard, 2001).
Funded by a Green Building Alliance grant from the state of Pennsylvania, an integrated LED luminaire is under development for commercial and residential applications. This daylight-mimicking system may reduce the symptoms associated with dementia in AD and increase sleep efficiency in individuals with sleep problems such as Delayed Sleep Phase Syndrome (DSPS) and Seasonal Affective Disorder (SAD). This luminaire is a retrofit fixture to easily replace the 2' x 2' fluorescent luminaire characteristically installed in the suspended acoustical tile ceiling systems of most commercial and institutional applications. The luminaire is made of white LED strips together with RGB LED modules that are capable of emitting the full spectrum of light from 450 to 700 nanometers. The white and RGB LEDs together will be "auto-tuned" to mimic the full spectrum of natural daylight. Additionally, the intensity of the blue spectrum can be increased to stimulate the circadian system and compensate for the decreased levels of blue light received by the photoreceptors of the aging eye. This LED luminaire will chronobioengineer an indoor environment to compensate for the elderly's loss of light reception and to mimic the ideal color-changing, daylit entropic natural environment where humans originally evolved with the goal of improving health outcomes for today's technological society.
The authors of this paper have been working with administrators, staff and caregivers at St. Francis Country House skilled-nursing facility to develop criteria for the design of the LED luminaire prototype. The prototype is being manufactured, will undergo UL-testing and, once approved, LED luminaires will be manufactured in quantities for installation on the fourth floor dementia unit there. While programmed to mimic daylight, the LED fixtures will be modifiable and can be "fine-tuned" in response to changes in resident behavior to achieve optimal outcomes. While it is being designed for the elderly and persons with sleep disturbances, there is great potential for other 24-hour environments that require people to work extended hours or night-shifts, for example at hospitals and factories. Additionally, this product would be useful in geographic locations that do not experience the characteristic diurnal lighting cycle of daylight hours and nighttime hours, such as is experienced in Alaska and other extreme latitude locations where there is a high incidence of seasonal affective disorder (AMA, 2012; Pail, 2011; Mills, 2007; Webb, 2006; Roberts, 2001; Rosenthal, 1985).
This luminaire will revolutionize the lighting industry by making an integrated daylight-mimicking LED luminaire commercially available to ameliorate sleep problems and global functioning for people who are affected by DSPS, SAD, AD, or other desynchronized biological rhythms, or those afflicted with dementia. Unfortunately, the development of disturbed sleep-wake rhythms, reverse day-night patterns, and agitation frequently result in institutionalization of persons with dementia. The use of therapeutic light to treat these symptoms has the potential to improve their quality of life (Royer, 2011; Sinoo, 2011; Burns, 2009; Van Hoof, 2009; Riemersma-van der Lek, 2008; Sloane, 2007; Torrington, 2007; Doliansky, 2006; Aarts, 2005; Schochat, 2000). If used in the home environment, this therapeutic light could possibly delay institutionalization and would improve the family caregivers' quality of life.
The architect John Eberhard has demonstrated the intimate relationship between architecture and neuroscience, especially with respect to sense perception and the cognitive experiences of humans with respect to space and place (Eberhard, 2009). A leader in basic and applied research specific to older adults, John Zeisel has identified the close relationship between environment, behavior and neuroscience to determine environmental design characteristics for Alzheimer's Special Care Units. His research correlates brain physiology with cognitive function to identify the performance criteria of spaces and possible design responses. For example, in addition to disruption of circadian rhythms, degradation of the SCN leads to a loss of the sense of time or season, which can be ameliorated by environments that provide contact with nature, such as gardens or even views to the outdoors (Zeisel, 2006). To provide seniors with an indoor environment with changing light conditions throughout the day would provide them with a more natural cue to the diurnal passage of time.
The daylight-mimicking luminaire will be installed at St. Francis Country House as a clinical trial and will be evaluated using Evidence-Based Design (EBD) research in collaboration with the Center for Health Design. EBD is the process of making decisions about the built environment on credible research to achieve the best possible outcomes. EBD considers the effect of the built environment on patient clinical outcomes in the areas of staff stress and fatigue, patient stress, and facility operational efficiency and productivity. The goal is to improve quality and patient safety. As defined by the Center for Health Design, EBD research is used to guide design of indoor healing environments and is based on research culled from the neurosciences, evolutionary biology, psychoneuroimmunology (effects of the emotions on the immune system), and environmental psychology (Malkin, 2012).
Funded by a Transform grant from the American Society of Interior Designers, this EBD research will be conducted in three phases. Phase One will collect baseline environmental data from the fourth floor dementia unit, to include: existing lighting levels in resident rooms, corridors and group activity rooms with respect to time of day, including nighttime; assessment of light conditions, including vertical and horizontal illuminances and color temperature; identify the reflectance values for ceiling, walls and floors; and identify different types of environmental light sources. Phase Two will collect data on the residents both pre- and post-installation of the lights. Information collected will include: schedule of resident daily activities, resident movement patterns/flow, general operations of the dementia unit, caregiver note taking and observations will be standardized, and data will be collected on pain medication dosages administered. Standardized checklists and tests will be used such as Activities of Daily Living (ADL), Mini-Mental Status Exam (MMSE) and Caregiver Strain Index (CSI). After 30 days of daily exposure to the LED lighting system, data will be collected on residents for Phase Three. Specific data will be collected using ActiWatches to monitor sleep/wake cycles. Standard tests will include the Pittsburgh Sleep Quality Index and Karolinska Sleepiness Scale, as well as a non-standard test to measure lighting system satisfaction.
EBD at St. Francis Country House will demonstrate the broader application of this daylight-mimicking luminaire to improve sleep and global functioning of individuals with dementia, which will open a lucrative market for this potentially FDA-approved luminaire for photobiology therapy. Additionally, the EBD research has the potential to impact current and forthcoming safety guidelines offered by the Illuminating Engineering Society (IES) as well as provide the Department of Energy with supporting data on the energy-efficiency of programmed LED luminaires for 24-hour facilities.
Conclusion
By developing new lighting systems it is possible to chronobioengineer the indoor environment to be in sync with the ideal color-changing daylit entropic natural environment out of which humans originally evolved. The goal is to improve health outcomes for today's technological society. It has been well-established that natural light and views to nature (Kaplan, 1995) are critical in reducing medication and the length of hospital stays (Torrington, 2007; Ulrich, 1984) and that morning light is beneficial for synchronizing circadian rhythms. However, it is not always possible to design all indoor spaces to be oriented to the cardinal directions to ensure optimal lighting conditions throughout the day, especially when a retrofit of existing conditions. Furthermore, there are no standards presently in the lighting industry for the photobiological, or non-visual aspects of light (Noell-Waggoner, 2004). Neither are there established guidelines for lighting levels or wavelengths, nor has the time of day light should be administered been precisely identified, nor for how long (Deschenes, 2009). Most concur that studies to date indicate the need for more comprehensive studies (Hanford, 2013; Royer, 2011). The goal of the EBD research at St. Francis Country House is to establish methods to artificially illuminate building interiors to create healing environments for the elderly and to establish guidelines to chronobioengineer the indoor environment through a programmed daylight-mimicking LED lighting system. By supporting the bio-technical integration of lighting with building interiors, this LED luminaire will support a paradigm shift in the design of the built environment, specifically the use of light to improve health, wellbeing and performance.
References
Aarts, M.P.J. and Westerlaken, A.C., 2005, 'Field study of visual and biological light conditions of independently-living elderly people, Gerontechnology 4(3): 141-152.
American Medical Association, 2012, Council On Science And Public Health Report 4-A-12 (http://www.ama-assn.org/assets/meeting/2012a/a12-refcomm-d.pdf).
Ancoli-Israel, S., Klauber, M., Jones, D.W., Kripke, D., Martin, J., Mason, W., Horenczyk, P. and Fell, R., 1997, Variations in circadian rhythms of activity, sleep and light exposure related to dementia in nursing home patients, American Sleep Disorders Association and Sleep Research Society, 20()1), 18-23.
ANSI/IESNA RP-28-07, 2007, 'Recommended Practice for Lighting and the Visual Environment for Senior Living,' Illuminating Engineering Society of North America.
Berry, L., Parker, D., Coile, R., Hamilton, D.K., O'Neill, D., & Sadler, B. , 2004, The Business Case for Better Buildings. Frontiers of Health Services Management, 21(1), 3-24
Berson, D.M., Dunn, F.A., and Takao, M., 2002, 'Phototransduction by retinal ganglion cells that set the circadian clock', Science 295, 1070-1073.
Brainard, G.C., Hanifin, J.P., Greeson, J.M., Byrne, B., Glickman,G., Gerner, E. and Rollag, M.D., 2001, 'Action Spectrum for Melatonin Regulation in Humans: Evidence for a Novel Circadian Photoreceptor', The Journal of Neuroscience 21(16), 6405–6412.
Brock, M.A., 1991, 'Chronobiology and aging', Journal of the American Geriatrics Society 39, 74-91.
Burns, A., Allen, H., Tamenson, B., Duignan, D., Byrne, J., 2009, 'Bright light therapy for agitation in dementia: a randomized controlled trial,' International Psychogeriatrics 21(4): 711-721.
Chevan, H., 1992, 'Good office design can keep both your workers and your bottom line healthy', Office Systems 9(12), 22.
Clapin-French,E., 1986, Sleep patterns of aged people in long-term care facilities. Journal of Advanced Nursing, 11, 57-66.
Costa, G. ,1996, The impact of shift and night work on health. Applied Ergonomics, 27(1), 9-16.
Davis, S. and Mirick, D.K. ,2006, Circadian disruption, shift work and the risk of cancer: a summary of the evidence and studies in Seattle. Cancer Causes and Control 17, 539-545.
Davis, S., Mirick, D.K. and Stevens, R.G. ,2001, Night shift work, light at night and risk of breast cancer. Journal of the National Cancer Institute, 93(20), 1557-1562.
De Lepeleire, J., Bouwen, L., De Coninck, L., & Buntinx, F. 2007, 'Insufficinet lighting in nursing homes, ' Journal of American Medical Directors' Association, 8(5): 314-317.
De la Sierra, A., Segura, J., Gorostidi, M., Banegas, J.R., de la Cruz, J.J., and Ruilope, L.M., 2010, 'Diurnal blood pressure variation, risk categories and antihypertensive treatment', Hypertensive Research, 33, 767-771.
Deschenes, C.L. and McCurry, S.M., 2009, Current treatment for sleep disturbances in individuals with dementia. Current Psychiatry Reports 11: 20-26.
DOE 2013. http://www1.eere.energy.gov/buildings/ssl/ (accessed 01-18-2013)
DOE, "Light at Night: the Latest Science," U. S. Department of Energy (2010) http://apps1.eere.energy.gov/buildings/publications/pdfs/ssl/ssl_whitepaper_nov2010.pdf
Doliansky, J.T. and Dagan, Y., 2006, 'A chronobiological approach in the treatment of sleep disturbances in Alzheimer's dementia patients', Harefuah 145(6), 437-440.
Eberhard, J.P., 2009, Brain Landscape: The Coexistence of Neuroscience and Architecture, New York, Oxford University Press.
Edelstein, E., 2008a, 'Building health', Health Environments Research and Design Journal 1, 54-59.
Edelstein, E., 2008b, 'Neuroscience can inform healthcare design', Building Design and Construction 49, 52.
Ehert, C.F., Groh, K.B., and Mienert, J.C., 1978, 'Circadian desynchronism and chronotypic ecophilia as factors in aging and longevity', Advances in Experimental Biology and Medicine 108, 185-213.
Ellis, E.V., Handly, N.B., McEachron, D.L., Del Risco, A., Baynard, M., 2011, 'Daylighting, Daylight Simulation and Public Health: Low-Energy Lighting for Optimal Vision/Visual Acuity and Health/Wellbeing,' Linköping Electronic Conference Proceedings, 57.
Ellis, E.V., 2000, 'Learning To Forget: Architectural Recreation, Spatial Visualization and Imaging the Unseen,' Architectural Theory Review 5(2), 44-60.
Ellis, E.V., 1999, 'The Visible and Tangible Eye,' Proceedings of the 87th Annual Meeting of the ACSA, 351-356.
Gibson, J.J., 1966, The Senses Considered as Perceptual Systems. Boston: Houghton Mifflin Company.
Halberg, F., Tamura, K., Cornelissen, G., 1994, Chronobioengineering toward a cost-effective quality health care. Frontiers of Medical and Biological Engineering, 6(2), 83-102.
Hanford, N. and Figueiro, M., 2013, Light therapy and Alzheimer's Disease and related dementia: Past, Present and Future, Journal of Alzheimer's Disease 33: 913-922.
Harrington, J. ,1994, Shift work and health – A critical review of the literature on working hours. Annals of the Academy of Medicine, Singapore 23(5): 699-705.
Hastings, M.H., Reddy, A.B., and Maywood, E.S., 2003, 'A clockwork web: Circadian timing in the brain and periphery in health and disease', Nature Reviews: Neuroscience, 4, 649-661.
Haus, E. and Smolensky, M. ,2006, Biological clocks and shift work: Circadian dysregulation and potential long-term effects. Cancer Causes Control 17: 489-500.
Joseph, A., 2006, 'The Impact of Light on Outcomes in Healthcare Settings', The Center for Health Design Issue Paper #2, 1-12 http://www.healthdesign.org/
Kaplan, S., 1995, 'The restorative benefits of nature: toward an integrative framework,' Journal of Environmental Psychology 15: 169-182.
Khalid, H., 2006, 'Embracing diversity in user needs for effective design', Applied Ergonomics 37, 409-418.
Kilbert, C., Sendzimer, J., Bradley, G. ,2000, Listen to your mother: Applying insights from nature is one way to green the industry. Alternatives Journal, 26(1): 38-42.
Malkin, J., 2012, 'A Visual Reference for Evidence-Based Design' The Center for Health Design: http://www.healthdesign.org/
McEachron, D.L., 2012, Chronobioengineering: Introduction to Biological Rhythms with Applications, Volume 1. Morgan Claypool, San Francisco, CA.
Miles, L. E. and Dement, W.C., 1980, 'Sleep and aging', Sleep 3, 119-220.
Mills, P.R., Tomkins, S.C. and Schlangen, L.J.M., 2007, The effect of high correlated colour temperature office lighting on employee wellbeing and work performance, Journal of Circadian Rhythms 5(2).
Mitchell, C., Zhang, J., Sigsgaard, T., Jantunen, M., Lioy, P., Samson, R. and Karol, M. , 2007, Current state of the science: Health effects and indoor environmental quality. Environmental Health Perspectives 15, 958-964
Noell-Waggoner, E. 2006, ''Age Wave' Demands Sea Change', Architectural Lighting 20 (7), 53-55.
Noell-Waggoner, E., 2004, 'Lighting Solutions for Contemporary Problems of Older Adults', Journal of Psychosocial Nursing & Mental Health Services, 42(7), 14-20.
Pail, G., Huf, W., Pjrek, E., Winkler, D., Willeit, M., Praschak-Rieder, N., and Kaspeer, S., 2011, 'Bright-light therapy in the treatment of mood disorders', Neuropsychobiology, 64, 152-162.
Pittendrigh, C., 1993, "Temporal organization: Reflections of a Darwinian clock-weather. Annual Review of Physiology", 55, 6-54.
Regestein, Q. and Morris, J., 1987, Daily sleep patterns observed among institutionalized elderly, Journal of American Geriatric Society, 35, 767-772.
Riemersma-van der Lek, R.F., Swaab, D.F., Twisk, J., Hol, E.M., Hoogendijk, W.J.G., and Van Someren, E.J.W., 2008, 'Effect of bright light and melatonin on cognitive and noncognitive function in elderly residents of group care facilities,' Journal of the American Medical Association 299(22): 2642-2655.
Roberts, J.E., 2001, 'Therapeutic Effects of Light in Humans,' Photobiology for the 21st Century. Valdenmar Publishing Company: Overland Park, Kansas.
Rosenthal, N.E., Sach, D.A., James, S.P., Parry, B.L., Mendelson, W.B., Tamarkin, L., and Wehr, T.A., 1985, 'Seasonal affective disorder and phototherapy', Annuals of the New York Academy of Science, 453, 260-269.
Royer, M., Ballentine, N.H., Eslinger, P.J., Houser, K., Ricard, M., Behr, R., and Rakos, K., 'Light Therapy for Seniors in Long-Term Care', 2011, Journal American Meical Directors Association, 1-4.
Rydeen, J., Erickson, P. and Lange, J., 2008, 'Built for brains', Industrial Engineer 40, 33-36.
Samet, J. M. and Spengler, J.D., 2003, Indoor environments and health: Moving into the 21st century, American Journal of Public Health, 93(9), 1489-1493.
Samis, H.V. and Capobianco, S., 1978, Aging and Biological Rhythms, New York, Plenum Press.
Samis, H.V. Jr., 1968, 'Aging: The loss of temporal organization', Perspectives in Biology and Medicine 12, 95-102.
Schochat, et.al., 2000, 'Illumination levels in ursing home patients effects on sleep and activity rhythms,' Journal of Sleep Research, 9: 373-379.
Sinoo, M.M., van Hoof, J., Kort, H.S.M., 2011, 'Light conditions for older adults in the nursing home: Assessment of environmental illuminances and colour temperature,' Building and Environment 46: 1917-1927.
Sloane, P.D., Williams, C.S., Mitchell, C.M., Preisser, J.S., Wood, W., Barrick, A.L., Hickman, S.E., Gll, K.S., Connell, B.R., Edinger, J., and Zimmerman, S., 2007, 'High-Intensity Environmental Light in Dementia: Effect on Sleep and Activity,' Journal American Geriatrics Society 55:1524-1533.
Torrington, J.M. and Tregenza, P.R., 2007, 'Lighting for people with dementia,' Lighting Research and Technology 39: 81-97.
Turner, P.L. and Mainster, M.A., 2008, 'Circadian photoreception: ageing and the eye's important role in systemic health', British Journal of Ophthalmology 92, 1439–1444.
Ulrich, R., 1984, 'View through a Window May Influence Recovery from Surgery', Science 224, 420-421.
Van Gool, W.A. and Mirimiran, M., 1986, 'Aging and circadian rhythms', Progress in Brain Research 70, 25-277.
Van Hoof, J., Aarts, M.P.J., Rense, C.G., Schoutens, A.M.C., 2009, 'Ambient bright light in dementia: effects on behavior and circadian rhythmicity,' Building and Environment 44: 146-155.
Van Hoof, J., Westerlaken, A.C., Aarts, M.P.J., Wouters, E.F.M., Schoutens, A.M.C., Sinoo, M.M., Aries, M.B.C., 2012, 'Light therapy: methodological issues from an engineering perspective,' Technology and Health Care 20: 11-23.
Van Someren, E.J.W., Kessler, M., Mirmiran, M. and Swabb, D.F., 1997, 'Indirect Bright Light Improves Circadian Rest-Acitvity Rhythm Disturbances in Demented Patients', Biological Psychiatry 41, 955-963.
Vujovic, N., Davidson, A.J., and Menaker, M., 2007, 'Sympathetic input modulates, but does not determine, phase of peripheral circadian oscillators', American Journal of Physiology- Regulatory, Integrative and Comparative Physiology, 295, R355-R360.
Wang, N., 2009, In broad daylight: An investigation of the multiple environmental factors influencing mood, preference and performance in a sunlit workplace, BiblioBazaar, Ph.D. Dissertation.
Webb, A.R., 2006, 'Considerations for lighting in the built environment: Non-visual effects of light,' Energy and Buildings 38: 721-727.
Wu, Y.H. and Swabb, D.F., 2005, 'The human pineal gland and melatonin in aging and Alzheimer's disease', Journal of Pineal Research 38(3),145-152.
Wu, Y.H. and Swabb, D.F., 2007, 'Disturbance and strategies for reactivation of the circadian rhythm system in aging and Alzheimer's disease', Sleep Medicine 8(6), 623-636.
Zeisel, 2006, Inquiry by Design, New York, W.W. Norton & Company, Inc.
